We Help Healthcare Facilities Break the Chain of Pathogen Transmission™
*Cycle times as fast as 2 minutes for vegetative bacteria.
How Our Approach Reduces Pathogen Transmission
Xenex’s patented Pulsed Xenon UV system is at the core of our Germ-Zapping Robot. Through our service and support, we can help you reduce microbial load in healthcare rooms/areas with our easy to integrate approach and LightStrike™+ Robot.
Xenex’s solutions include training and advanced workflow consulting to help you speed room turnover and improve throughput. We collaborate with visionary clinicians and leading scientific experts around the world to fuel continuous improvement.

Committed to Evidence-Based Science
Xenex founders Mark(Tuck) Stibich and Julie Stachowiak met at Johns Hopkins University during their doctoral studies. Both epidemiologists, they had a shared passion for research and wanting to make the world a better place. They wanted to provide healthcare facilities with a more effective approach to prevent pathogen transmission, and they wanted to ensure that scientific evidence drove all of the company’s claims. In 2008, Tuck and Julie co-founded Xenex. Their passion became our mission and it remains the foundation of everything we do.
I Am Visionary
Meghann Holmes, RN, CIC & Samantha Green, RN
Infection Preventionists
We added Xenex LightStrike Robots to enhance our disinfection process and continue our mission to make patient safety a top priority. The results we achieved were really amazing.
*Associated with non-medical device products

I Am Visionary
Necia Kimber, RN, BSN, MHA, CIC
Infection Control & Prevention
We saw the greatest reduction of C. diff in the environment after integrating Xenex and the LightStrike robots into our disinfection bundle.
*Associated with non-medical device products

I Am Visionary
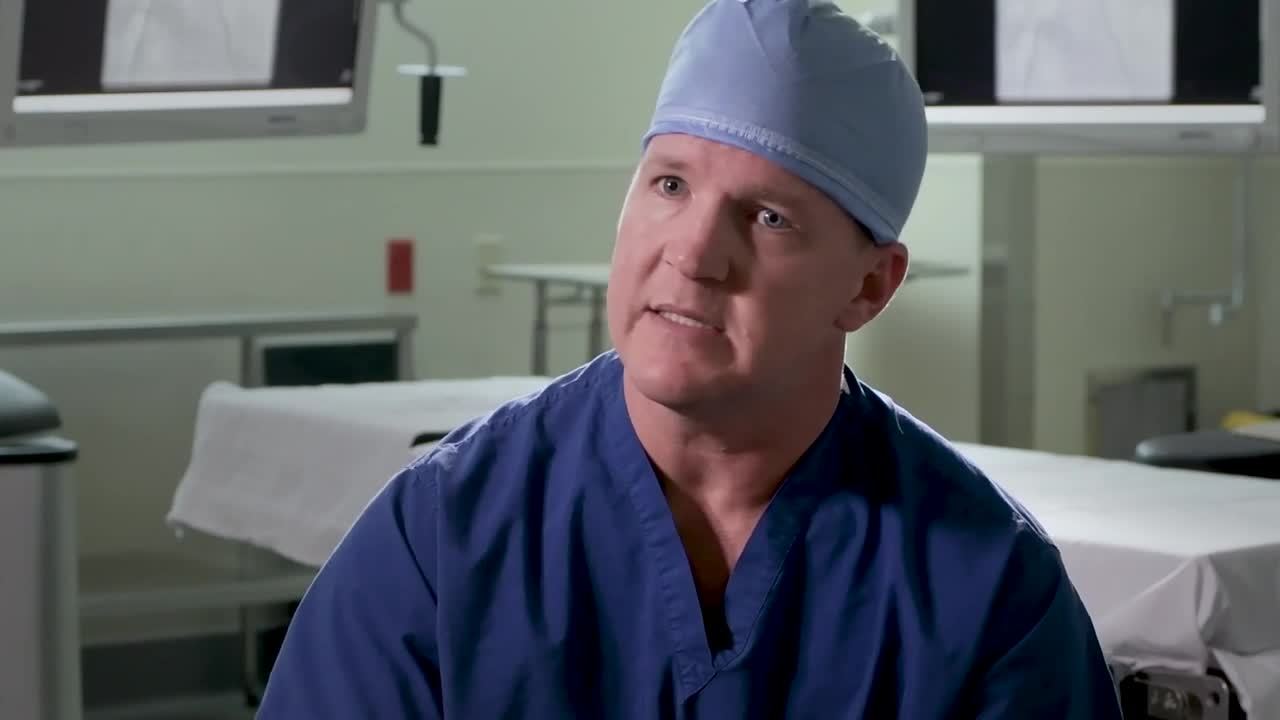
James Neel, MD
Cardiothoracic Surgeon
The LightStrike Robots are an effective tool in our battle against pathogens and provide us with an advantage in the surgical suite.
*Associated with non-medical device products

I Am Visionary
Kristin Pickerell DNP, RN, NE-BC, CPHQ
Director of Quality
Xenex has a very strong data support team and that has been instrumental to show we are making a difference.
*Associated with non-medical device products

I Am Visionary
Mark Povroznik, Pharm.D.
VP/Chief Quality Officer
We switched from Mercury UV to Xenex LightStrike Robots to improve our quality program and increase throughput.
*Associated with non-medical device products

I Am Visionary
Dorian Williams, FACHE, MHA, LSSBB
Assistant Vice President of Operations
We took our quality program to the next level by adding Xenex and their LightStrike Robots to reduce pathogens at our facility.
*Associated with non-medical device products

Xenex® Empowers Partners Committed to Microbial Reduction





*Customers using prior version non-medical device products.